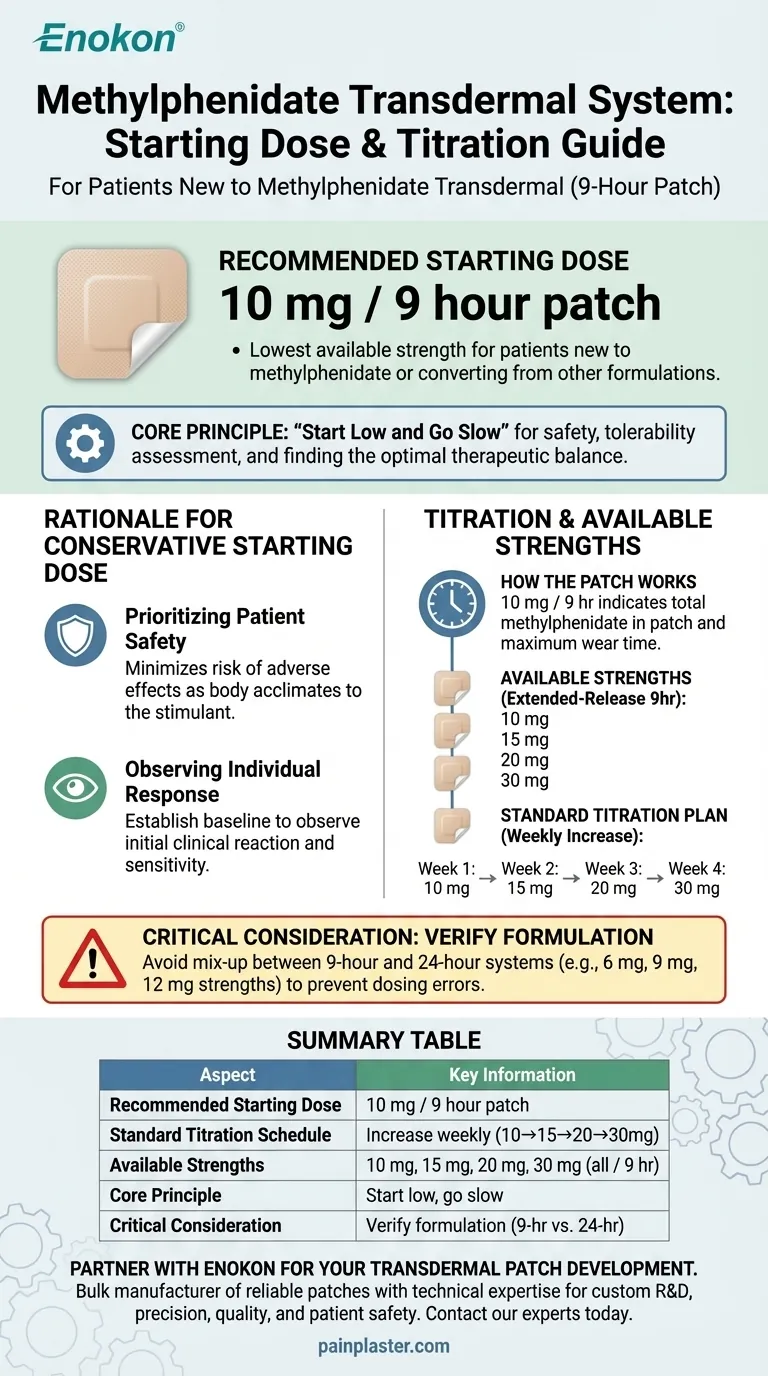
For patients new to methylphenidate transdermal systems, the recommended starting dose is the 10 mg / 9 hour patch. This initial dosage is the lowest available strength and applies to patients who have never taken methylphenidate before as well as those converting from other formulations. The patch is designed to be worn for a period of nine hours.
The core principle of initiating methylphenidate transdermal therapy is to "start low and go slow." Beginning with the 10 mg patch allows clinicians to safely assess a patient's response and tolerability before gradually increasing the dose to find the optimal balance between therapeutic benefit and potential side effects.

The Rationale for a Conservative Starting Dose
Initiating treatment with the lowest available dosage is a foundational practice in pharmacology, designed to maximize safety and effectiveness.
Prioritizing Patient Safety
A 10 mg starting dose minimizes the risk of adverse effects as the patient's body acclimates to the medication. This is especially critical for a central nervous system stimulant like methylphenidate.
Observing Individual Response
Every patient metabolizes medication differently. Starting low provides a clear baseline to observe the initial clinical response and identify any sensitivity to the drug before committing to a higher dosage.
Understanding the Dosing and Titration Schedule
The methylphenidate transdermal system is not just about the starting dose; it involves a structured plan for application and dose adjustment.
How the Patch Works
The dosage, such as 10 mg / 9 hr, indicates the total amount of methylphenidate in the patch and the recommended maximum wear time. The medication is released at a controlled rate over these nine hours.
Available Patch Strengths
The most common extended-release transdermal system is available in four strengths, allowing for precise dose adjustments:
- 10 mg / 9 hr
- 15 mg / 9 hr
- 20 mg / 9 hr
- 30 mg / 9 hr
The Standard Titration Plan
After initiating treatment, the dose may be increased on a weekly basis according to the patient's needs and response. A typical schedule is as follows:
- Week 1: 10 mg patch
- Week 2: 15 mg patch
- Week 3: 20 mg patch
- Week 4: 30 mg patch
This gradual increase allows clinicians to carefully find the most effective dose for the individual.
Critical Consideration: Verify the Formulation
A common point of confusion arises from the existence of different methylphenidate patch formulations on the market. Prescribing the wrong starting dose due to a product mix-up can lead to significant safety issues.
The 9-Hour vs. 24-Hour System
While the 10 mg / 9 hr system is common, other products exist. For example, some formulations are designed for a 24-hour wear time and have entirely different strengths, such as 6 mg, 9 mg, and 12 mg.
The Importance of Precision
Applying the dosing logic of one system to another is a critical error. A 10 mg dose in a 24-hour system would have a very different effect than in a 9-hour system. Always confirm the specific product and its approved dosing schedule.
Applying This to Clinical Practice
The goal is to initiate therapy safely while moving methodically toward the optimal therapeutic dose for the patient.
- If your primary focus is initiating therapy for a new patient: Begin with the 10 mg / 9 hr patch and adhere to the weekly titration schedule based on clinical evaluation.
- If your primary focus is converting a patient from an oral formulation: The starting dose remains 10 mg / 9 hr, as transdermal absorption profiles differ from oral medication.
- If your primary focus is avoiding medication errors: Always verify the specific brand and formulation (e.g., 9-hour vs. 24-hour system) before determining the starting dose and titration plan.
Ultimately, precise product identification and a conservative initial dose are the cornerstones of safe and effective treatment.
Summary Table:
| Aspect | Key Information |
|---|---|
| Recommended Starting Dose | 10 mg / 9 hour patch |
| Standard Titration Schedule | Increase weekly (e.g., 10mg→15mg→20mg→30mg) |
| Available Strengths | 10 mg, 15 mg, 20 mg, 30 mg (all / 9 hr) |
| Core Principle | Start low, go slow to assess tolerability and efficacy |
| Critical Consideration | Verify formulation (e.g., 9-hour vs. 24-hour system) to avoid dosing errors |
Partner with Enokon for Your Transdermal Patch Development
As a bulk manufacturer of reliable transdermal patches and pain plasters, Enokon provides healthcare and pharma distributors and brands with the technical expertise needed for custom R&D and development. Ensure your methylphenidate or other transdermal products are developed with precision, quality, and patient safety in mind.
Contact our experts today to discuss your specific project requirements and benefit from our manufacturing excellence.
Visual Guide
Related Products
- Menthol Gel Pain Relief Patch
- Silicone Scar Sheets Patch Transdermal Drug Patch
- Far Infrared Heat Pain Relief Patches Transdermal Patches
- Icy Hot Menthol Medicine Pain Relief Patch
- Mugwort Wormwood Pain Relief Patch for Neck Pain
People Also Ask
- What are the different types of pain relief patches available? Find the Right Solution for Your Pain
- When should you consider using pain relief products like creams and patches? Optimize Comfort & Safety
- What safety considerations should be kept in mind when using pain relief patches? Ensure Safe & Effective Pain Management
- What are pain relief patches and how do they work? Discover Non-Invasive Pain Management
- How do pain relief patches compare to other pain relief methods? Discover Targeted, Long-Lasting Relief